[While there is good reason to be concerned about and address potential negative impacts of presence, especially when fast-evolving technologies including artificial intelligence are involved, there are also many potential positive impacts. This story from R&D World describes some extremely important positive impacts in the context of telerobotic surgery. See the original version of the story for a larger version of the graphic below and five additional images. –Matthew]
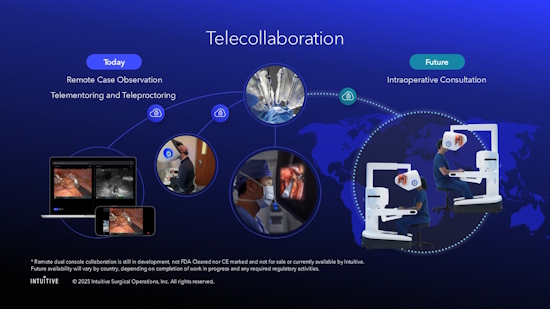
[Image: Intuitive’s telecollaboration roadmap spans today’s remote case observation and telementoring to a future vision of intraoperative consultation, where a remote surgeon could join a live case from a second console. Remote dual console collaboration is still in development and not yet FDA cleared. Credit: Intuitive]
A surgeon and Intuitive exec explain what da Vinci 5’s 10,000x computing leap actually looks like, inside and outside the OR
By Brian Buntz
April 1, 2026
Minutes after stepping off a Southwest flight in San Jose, the surgeon Douglas Stoddard, Director of Surgery and Robotics, CHRISTUS Health, was in an operating room in San Marcos, Texas. His colleague had an elderly woman on the table with a perforated gastric ulcer, a case he had always done open, meaning a large incision, ten days in the hospital, and what Stoddard described as a meaningful chance of not making it. Stoddard pulled up a chair at the gate, connected through Intuitive’s telepresence system on the da Vinci 5, and talked him through port placement and the repair in about 30 minutes, he explained. “You took the fear away from me,” his colleague told him afterward. The patient went home the next morning.
Stoddard told that story the following day on stage at NVIDIA GTC 2026, alongside Tony Jarc, VP of Digital and AI/ML, Intuitive. Intuitive now has more than 12,000 systems in hospitals globally and says more than 20.4 million cumulative procedures have been performed using its technology, roughly 8,700 a day. Da Vinci 5, the latest-generation system, delivers 10,000 times the computing power of its predecessor, the da Vinci Xi, with computing architecture built in partnership with NVIDIA using technologies including the Blackwell platform, Clara, and Omniverse. The added compute supports new capabilities, including force sensing at the instrument tip. Intuitive’s Case Insights platform uses da Vinci system data, video, and kinematic movement data to provide post-procedure analytics with machine-learning phase segmentation and objective performance metrics.
Before da Vinci 5, Stoddard said, feedback after a surgery could be something of an enigma. He recalls a supervising surgeon who would yell at him mid-case, then put an arm around him afterward and say, “Well, Doug, that went well. Let’s get some soup.” That was the debrief. The Xi generation let him pull down video to a hard drive, but the process was unreliable and rarely worth the effort. “Before DV5, I don’t think I could have found the spot in the video to review,” he said.
Those three data streams, system telemetry, video, and kinematics, feed into Case Insights, which translates raw, unstructured information into navigable performance analytics. “We’re now able to measure things in surgery that we weren’t able to measure before, like forces,” Jarc said. “We’re able to take unstructured data from all these procedures and organize it through a language of surgery so surgeons can interpret it.” The system’s algorithms identify what step of a procedure a surgeon is in, what anatomical structures are in the scene, and what clinical milestones have been reached, what Intuitive’s own literature calls machine-learning phase segmentation.
While surgery is a mix of art and science, Stoddard sees tools such as the da Vinci 5 leading to a pronounced shift in how surgeons review procedures. “Surgery is always going to have a degree of artfulness to it,” Stoddard said. “But if you want to decrease quality variance at scale, you need quantifiable science linked to outcomes that you can scale to everybody.”
Stoddard compared surgical training to a kung fu lineage. “You can almost watch a surgeon operate and trace them back to who trained them initially, because it’s that closed,” he said. “You learn, you operate, you teach. And you’re in this bubble within the four walls of an operating room.” When a surgeon hits a problem, they invite a colleague to help. “Sometimes they’re available, sometimes they’re not. And the patient gets what the patient gets.” Tools like da Vinci 5 and Telepresence break that pattern. “It has been unthinkable in surgery, until now, to be able to tap this pool of knowledge globally, immediately, so that you’re no longer limited to the lineage in which you were taught.”
A late-1990s American Board of Surgery study found the average general surgeon performed about 398 surgeries per year, a figure that remains a widely cited benchmark for per-surgeon volume. While volumes vary considerably, over a full career, most surgeons end up providing care to thousands of patients. Jarc sees AI providing something of a multiplier effect for a given surgeon. “Imagine that surgeon can help train 300 additional surgeons and transfer that technique, so they don’t have to go through the same learning curve or same experimentation,” he said. “All of a sudden, that one surgeon reaches 140,000 patients.” Scale that to a global community of 100,000 trained surgeons all collaborating, he argued, and “surgery is going to be this never-ending discovery mechanism.”
Stoddard framed the same ambition from the data side. “We want hundreds of thousands, millions, of hours of surgical video that AI is interpreting from across the globe for this particular procedure,” he said. “Applying knowledge you could only get across thousands of lifetimes as a surgeon, ten, a hundred, ten thousand,” he said, using the figure as illustrative of a scale no individual surgeon could match. “Finding insights in the details of how I’m operating that would be impossible for me to understand as an individual, and providing those insights on demand, every time.”
The gallbladder on the phone
Stoddard described a recent gallbladder removal where the tissue tore. Before da Vinci 5, he said, answering why would have been guesswork. “If I don’t have the video available through DV5, and I don’t have the ability to analyze forces during the case, I’ll have a really difficult time answering that question well.”
With the new system, he went back. “I didn’t love how that felt. I’m going to go back to that case and look at the force feedback components. I’m going to use the AI-interpreted video segments and skip straight to taking the gallbladder off the liver bed.” He pulled up the force data, found the peaks, and matched each one to what he was doing in the video. “Which parts had the highest spikes? I go to each spike and ask: What was I doing at that moment? How was I holding the gallbladder? Was I even paying attention to it with my left hand where the spike was?”
The answer was clear. “I should have turned my hand a little this way. I can see in the video it was here, and that’s where the force resulted in a tear.”
The next case, he said, he found himself in the same moment, and held the tissue differently. “I look down at my display, and there’s a force gauge. As the gauge approaches the level where I know I tore it last time, I stop myself, readjust, grab differently, and I don’t tear the gallbladder.” He called the shift not incremental but “transformative, groundbreaking, paradigm-shifting.” And he is more than 1,000 robotic procedures in.
Replacing surgical “gut feel” with quantifiable data
The gallbladder case is one data point in a broader shift. For decades, surgical feedback has run to a degree on instinct, sometimes being “more of an art” than a science, as Stoddard puts it. “Having a safe benchmark to hang onto as surgeons is so different from what we did before,” he said. “It was so much more of a felt sense. An ‘Oh, this feels right’ instinct.” He is blunt about the dangers of overreliance on a kinesthetic sense. “That’s how you have one good day and one bad day. You want all good days.”
The shift is still early, and force measurement is one of its clearest test cases. In emergency procedures involving fragile, dilated bowel, cases many surgeons avoid doing minimally invasively, Stoddard has started building his own thresholds. “A great example: small bowel obstructions. When you have hugely dilated loops of bowel that are very fragile, surgeons are terrified to operate minimally invasively. From a laparoscopic standpoint, you’re afraid laparoscopic instruments will tear that bowel… Anecdotally, I’ve realized I want to keep the force below about four to five Newtons,” he said. “I can see that because it’s just past halfway on the force gauge. I can feel the feedback in my hands and stop pulling and readjust my grip.” But he is careful not to oversell the number. “Is that four-to-five Newton threshold a proven number? No. We need a lot more volume for that.” Jarc drew the same boundary around the broader effort to link instrument forces to patient outcomes.
Still, both Jarc and Stoddard see more potential to continue redefining surgery. “Right now, if any of us in this room had a surgical disease, your ability to get through that disease and live the best possible life is exceptionally variable,” Stoddard said at GTC. “It depends on the disease itself, but it also depends on where you happen to be, what hospital you’re going into, the skill set of the surgical team, and the resources they have available. Sometimes that matters more than the disease process itself.” The global numbers bear that out: a multinational study in the British Journal of Surgery found that postoperative mortality is roughly three times higher in low-income countries than in high-income ones, even after adjusting for patient risk. Life expectancy between the two groups differs by roughly 15 years.
Closing that gap, Stoddard said, is the ultimate promise of pulling surgical data out of the dark. It is about allowing surgeons across the globe “to provide, in a more consistent way, every time we put knife to skin, the very best version of ourselves.”
Achieving that consistency, however, will require a continued evolution of surgical workflows. Stoddard warned against taking these new capabilities and simply applying them to the mindset of traditional laparoscopic surgery. Instead, the influx of data is prompting surgeons to rethink procedures that have long been done in much the same way.
More than a decade ago, Dr. Richard Satava, a former DARPA program manager whose program funded the telepresence surgery work at SRI International that laid the groundwork for the original da Vinci system, opined at FutureMed in 2012 that 95% of the early surgical robot’s potential was being squandered because the data it generated was simply thrown away. Satava, himself a flight surgeon and Army astronaut candidate, saw the robot as an information system.
Now the dream of data feeding back across the entire healthcare enterprise the way a fighter pilot’s avionics feed a post-mission debrief has come to fruition. “Patients put their lives in our hands,” Stoddard said. “We’re not only going to squeeze every drop out of that tool, but we are going to fly that plane till we break the damn wings off. We want to know every left and right boundary, and we are just going to go at it as surgeons, because we want every drop that we can get out of this technology for our patients.”
Leave a Reply